Rehab economics
Let’s talk about one of the big underlying problems with back pain, rehab and recovery, and put on our Planet Money caps so we can talk a bit about the economics behind it.
The symptom: many patients going through rehab are not incentivized to go through rehab, drop out, and cost the health care system a lot more later on.
The underlying problem: Rehab is priced incorrectly, both at the individual incentive level and at the health care systems level.
Let’s go through in detail why this problem exists.
At the individual level, patients quit rehab for the same reason that anyone quits something difficult: because they’re not sufficiently incentivized to continue.
Generally speaking, there are two kinds of incentives to do rehab (after all, it’s a lot of work).
-Personal incentives (my back hurts, my quality of life is low as a result);
-Economic incentives (My insurance will reimburse me for up to X visits to a therapist).
Generally speaking, personal incentives are good for getting people to start rehab, but less good at getting them to follow through with the hard part: actually sticking with it. This is where economic incentives have the potential to play a key role. (As a good analogous example: if you want to get people to quit smoking, pay them.)
Why aren’t personal incentives sufficient? Isn’t back pain a bad thing? Yes, it is- but humans are inherently very poor at staying motivated when outcomes are delayed and uncertain. Rehab is hard, and it takes time for you to see results. When people can’t visualize their progress, and see that their effort is paying off, their personal incentive to invest the effort wears off. Many of them quit, and cost the system more money later.
Why, then, can’t payers and providers (who have the most to lose economically when patients don’t recover) simply increase the economic incentive, i.e. the amount they are willing to pay for patients to follow through with their rehab? If disability is so expensive, why aren’t we paying patients to stick with their recovery plan, like we’re now doing for quitting smoking?
To answer that question, you have to look at the system level why payers should incentivize rehab at all:
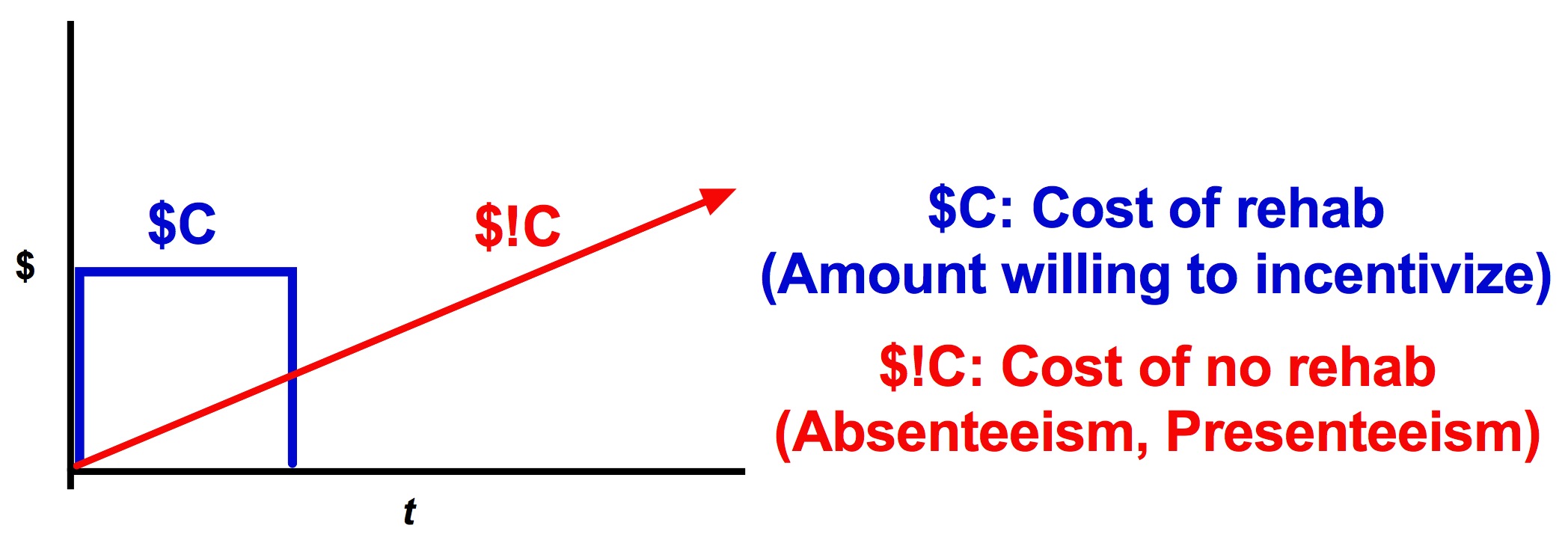
Payers incentivize rehab ($C) because it reduces their exposure to $!C: absenteeism, presenteeism, and the other insidious costs of disability.
Here is the problem with this setup, and why you can’t simply increase $C:
- Payers spend $C to reduce exposure to $!C.
- $!C is unpredictable, and highly variable patient to patient over time.
- $C is priced statically. (‘We reimburse up to $X’).
The end result? One-size-fits-none pricing of $C. This doesn’t work very well.
To see why this is such an inefficient use of $C, consider three hypothetical patients:
Patient A, a healthy young person with an elbow injury but who otherwise will not cost much in $!C. Since $C is likely > $!C, the payers are exposed to overpaying for $C.
Patient B, a person in their 60s with a nagging knee injury that has always been problematic, and whose $!C costs have added up over the years. Since $!C is likely > $C, payers are exposed to $!C costs due to inadequate or incomplete rehab.
Patient C, someone in their 40s entering the prime of their working career with a bad back that seems to get worse every year. They’re about to go on long-term disability from work, and could cost the system millions in $!C down the road. Here, $$$!C >>> $C, and payers are highly exposed to long-term costs unless corrective action is taken immediately through intense rehab.
You can see the problem with one-size-fits-none: increasing $C allowances across the board for a small amount might help lower total costs for Patient B, but will probably make patients A and C more expensive long-term (patient A didn’t need more care anyway, and for patient C a small increase in spending won’t matter). Payers ultimately get burned, mostly from high exposure to $$$!C from patient C.
So how could you fix this problem? One way would be to try giving patients more real-time information and feedback about their recovery, in order to preserve personal incentive for longer. That could potentially work, but wouldn’t radically change the way we incentivize and pay for rehab.
A more interesting way might be to give payers information that will allow them to price $C as a function of anticipated $!C on an individualized level, allowing economic incentives to kick in powerfully, but only when necessary. If your rehab is going fine, that’s great. But if it’s not, kicking in a few dollars in incentive money now could make a big difference in savings later on.
Figuring out exactly what that information is? That’ll be the interesting part. Whoever can figure that out will have a really interesting business model to work with, and a shot at making big changes to the way we price rehab.
