A problem with science: Disruptive vs. Sustaining Research
Over the past three years, as I’ve spent time in a wonderful lab full of exciting and supportive people doing research I greatly enjoyed, I’ve had to think a great deal about why exactly I feel so compelled to make an early exit from academic science. The main reason has to do with researchers’ incentives, and why those incentives are increasingly setting researchers up for frustration and failure.
Let’s start with the basic assumption that the purpose of life science research is to improve health care by advancing our understanding of the human body in health and disease. This is a broad statement, but it is worth considering why exactly improving our understanding of health and disease mechanisms will lead to improved patient outcomes for lower cost. Clayton Christensen, the well-known author of The Innovator’s Dilemma (the groundbreaking book about disruptive technology), addresses this in his follow up book, The Innovator’s Prescription: a Disruptive Solution for Health Care. One of the authors’ important points is that medical conditions can be categorized based on two criteria: the extent to which we understand the underlying micro-mechanisms of the disease, and the effectiveness of current available treatments.
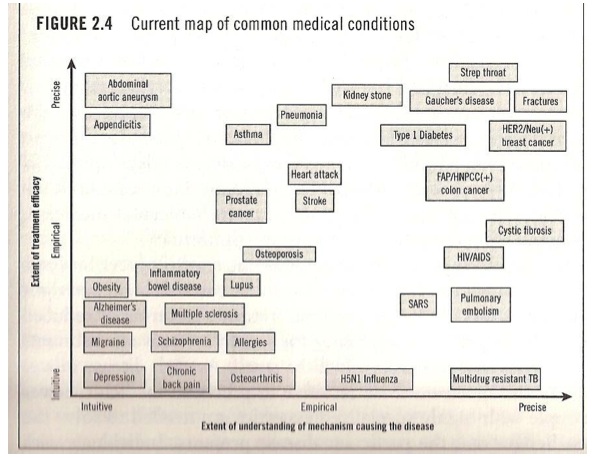
We can see graphically in this figure from the book that diseases tend to cluster in three areas. The upper right hand corner of ‘Precise understanding + Effective treatment’ (Fractures, strep throat, Type 1 diabetes, many infectious diseases) he calls Precision Medicine. These are conditions with specific, reliable diagnoses and (usually) straightforward treatment courses. In the lower left hand corner, on the other hand, we see the opposite: little/no mechanistic understanding along with ineffective, usually expensive treatment options. Here is where we find many of the largest burdens on health care: depression, Alzheimer’s disease, low back pain, obesity, and so forth. He calls this region Intuitive Medicine: diagnosis and treatment are highly inexact, and mostly rely on the clinician’s intuition and past experience; few if any treatments have ever been demonstrably successful in a clinical trial. In the middle, we have intermediate conditions that are partially understood, and where diagnoses and treatments cannot be pronounced with certainty but can be given with a good probability of being correct. Diseases in this area (osteoporosis, heart disease, stroke, prostate cancer) are not precisely but are at least empirically understood; therefore the authors call this field Empirical Medicine.

In The Innovator’s Prescription, Christensen argues that one of the best ways to improve health care while reducing costs is to move specific diseases from Intuitive to Empirical and finally to Precision Medicine through scientific research. This is a fairly straightforward concept. Consider the following: back when we did not have a precise understanding of infectious diseases, simple infections used to kill hundreds of thousands of people a year in the developed world, whereas they are now relatively simple and straightforward to treat with a course of antibiotics. Why? Because we have successfully moved simple infections from Intuitive to Precision medicine through scientific research. The discovery of microorganisms and subsequent development of antibiotics allowed us to move many infections diseases off of the red trajectory in the image above down to the blue trajectory: the potential for treatment success went from limited to extremely high due to this shift. Now think about low back pain. Back pain is an enormously expensive burden on our health care system, as many people are affected by it and our understanding of the underlying causes is extremely limited. Our treatment options are often ineffective, and patients do not get better: low back pain is ‘stuck’ on the red trajectory as a chronic disease in the realm of Intuitive Medicine.
It seems clear to me that the broad goal of life science research should be to ‘move the boxes’: to bring a condition like low back pain towards empirical medicine and hopefully one day towards precision medicine. Yet, our understanding of many of the most crippling and burdensome diseases in intuitive medicine has made shockingly little progress over the last few decades, despite a great deal of research investment. (Think about how much time, effort and money has gone into research on mental illness. Our frustrating lack of research progress isn’t for lack of effort.) I believe that the reason we have made such little progress in these areas is not because we haven’t moved the boxes: it’s because we haven’t been moving the boxes in the right direction.

In my opinion, scientific research has the potential to move boxes in two distinct ways. Borrowing terms from the Innovator’s Lexicon, I call one ‘disruptive research’, and the other ‘sustaining research’. Disruptive research accomplishes what we would like research to accomplish: to introduce new ways of thinking about a disease or a treatment strategy, and to challenge our assumptions about what we think we know. Disruptive research often confronts the research crowd head on: it comes out of creative, cross-disciplinary studies that challenge traditional ‘truths’ about isolated disciplines, as well as from ‘crazy, moon-shot ideas’ that are dismissed and ridiculed by everyone else, and then radically transform (or at least challenge) the research establishment. This is the type of research that can move a Disease Box from one trajectory to another: if a box is stuck on one path, it takes some disruptive science to get it unstuck and bumped down into a faster track.

Sustaining research, on the other hand, moves boxes forward but along the same lines. Sustaining research does not meaningfully challenge any assumptions; it simply ‘adds knowledge’. Each individual experiment or publication may appear to contribute something of value to the field, but the net effect of sustaining research is to make it harder for disruptive research to occur. The farther you are along the red line, the harder it is to drop all the way back down to the bottom of the purple line; yet, that is exactly what has to be done to achieve true research progress. A vast number of publications, funded grants, and even entire careers have been built on sustaining research: yet, their net effect may have been more negative than positive for health care as a whole.
There is another aspect of sustaining research worth mentioning: it tends to be not much fun. I sometimes refer to sustaining research as ‘trench warfare’ because that’s what it can feel like. Adding knowledge in a sustaining manner can be utterly exhausting: as more and more gets published in a research field, the remaining questions that need answering become progressively more challenging to address experimentally. The introduction of cutting-edge technology and fancier lab equipment does not change this paradigm, but instead accelerates it, allowing for more and more research dollars to be converted into publications without moving any disease boxes in a disruptive direction. As lab research technology continues to evolve at a faster and faster rate, the publication/funding/publication cycle turns into a rat race, which can be pretty miserable.
If sustaining research is so stressful and does not meaningfully contribute to health care progress, then why do so many of us willfully engage in it? I believe that the reason so many people turn to sustaining research is that all of the incentives currently point that way. You might ask, is that really the case? Isn’t the goal of every scientist to cure a disease and revolutionize a field through several brilliant and creative papers in Nature or Science? Well, sure, in theory. But in real life, the most immediate and powerful motivating factor for academic scientists is to acquire, maintain, and not lose their grant funding. Grant funding is critical to lab operation, but the ratio of funded to unfunded grants has been in free fall for the last twenty years. The percentage of research grants awarded to young investigators at the start of their careers is dropping as well, and without funding, a young researcher’s career will be over quickly. The situation a junior professor faces can be summed up as follows:
1) There is strong pressure from your university (i.e. employer) to get as much funding as quickly as possible.
2) To get and maintain grant funding, you need to start publishing your research findings in peer-reviewed journals as quickly as possible.
3) To get publications, you need results. Negative results won’t cut it.
4) To get results, you need grant funding to pay for the lab, personnel, and experiments.
5) You really, really don’t want to lose your faculty position.
Unfortunately, these pressures do not combine well with the sort of creative, cross-disciplinary thinking that leads to disruptive research. For starters, the committees who allocate federal grant funding dollars (from the NIH in the United States, CIHR or NSERC in Canada, or other large funding bodies) tend to judge grant applications based on the research background leading up to the proposal, the plausibility of success and the track record of the applicants, all of which contribute to the notion of how ‘safe an investment’ each proposal appears to be. Creative proposals that reach across various disciplines and do not follow the molds cast by the body of existing research tend to not do so well by these criteria. As a result, applications to fund sustaining research have a much better chance of success than applications to fund disruptive research. This imbalance helps to perpetuate the cycle of sustaining research leading to even more sustaining research without meaningfully improving health care.
Unfortunately, there is another even more powerful barrier to disruptive research that is an inherent trait of science itself. Radical ideas, no matter how creative, cross-disciplinary or groundbreaking they may be, usually don’t succeed experimentally. That’s why they’re radical ideas, after all: they’re akin to a high-risk high-gain investment or a gambling wager against long odds. These high-risk strategies can pay big dividends, but it’s probably best not to bet your entire life savings this way- the potential consequences will be felt very personally and painfully. Unfortunately, as a young researcher, focusing your research program on creative, potentially disruptive scientific problems is a little bit like mortgaging your house to play the lottery. Yes, you might make a huge scientific breakthrough, and move a box in the right direction on our health care graph. On the other hand, you probably won’t.
The riskiness of disruptive research can be felt at nearly every stage in a scientist’s career, but it is most apparent precisely at the point of peak creativity: with postdoctoral fellows and junior faculty members. For those who don’t know, postdocs are researchers who have just finished their PhDs and who join an established lab for a few years to independently work on projects and acquire some publication muscle. In many large research groups, postdocs do a lot of the actual lab work, and form a critical part of the research ecosystem. However, when choosing how to allocate postdoc labor, the senior researcher in charge of the lab has an unpleasant choice: whether to play the odds and pursue disruptive research questions, or to play it safe with the same old sustaining stuff. If you choose the risky option and send out 10 postdocs with disruptive projects, then one of them might come out with a Nature paper and get a faculty position at Stanford- but the other nine are out of luck. The dice didn’t roll their way, and they either need to take on another postdoc position or start looking at alternate careers. Sound scary? Well, it is scary- and it’s a huge incentive to stick with safe, sustainable research where everybody gets a paper and no one gets left out, even if those papers don’t really change much in the grand scheme of things. Also- remember that one postdoc who got lucky, scored a big disruptive finding, and got a job at Stanford? He’s now a junior faculty member writing grant proposals, and feeling the pressure to fall in line with sustaining proposals. The odds are stacked against disruptive science, every step of the way.
I’m hardly the first person to suggest that the academic research ecosystem is approaching a breaking point, as others have outlined in much greater detail. Personally, I think this problem is inherently fixable, but will require some creative thinking that isn’t simply ‘we need more funding’. I’ll save my thoughts on those solutions for a future post.
